Amoebiasis is the second leading cause of death from parasitic disease worldwide.
Entamoeba histolytica has a simple lifecycle, existing as either the infectious cyst form or the amoeboid trophozoite.
Human beings, and perhaps some non-human primates, are the only natural hosts.
Infection usually begins with the ingestion of the cysts in food or water that has been contaminated by human faeces.
Entamoeba histolytica cysts are inert, round and are surrounded by a refractile wall that may include chitin.
They survive the acid of the stomach, travel through the small intestine, and, within the terminal ileum or colon, excyst to form the trophozoite.
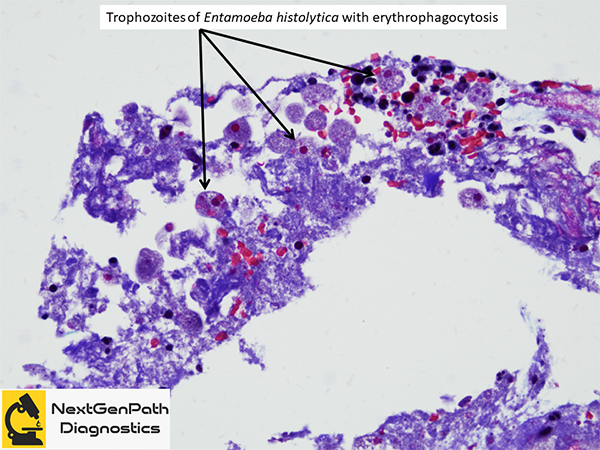
Entamoeba histolytica trophozoite invades the intestinal mucosa by secreting proteinases that dissolve host tissues.
Trophozoites ingest blood cells, bacteria and food particles, reproduce by binary fission, and encyst within the colon, completing the lifecycle when infectious cysts are excreted into the environment in stool.
In some cases amoebae breach the mucosal barrier and travel through the portal and systemic circulation.
Many individuals with Entamoeba histolytica infection have no symptoms, and can clear their infection without any signs of disease. However, 4–10% of asymptomatic individuals develop disease over a year.
Patients with amoebic colitis present with bloody diarrhoea, abdominal pain and tenderness.
The onset is often gradual, with patients reporting several weeks of symptoms. Multiple small volume mucoid stools are common (mimicing inflammatory bowel disease) but profuse, watery diarrhoea might be noted (mimicking microscopic colitis).
Rectal bleeding without diarrhoea may be seen, especially in children.
The diagnosis of amoebic colitis rests on the demonstration of Entamoeba histolytica in the stool or colonic mucosa of patients with diarrhoea.
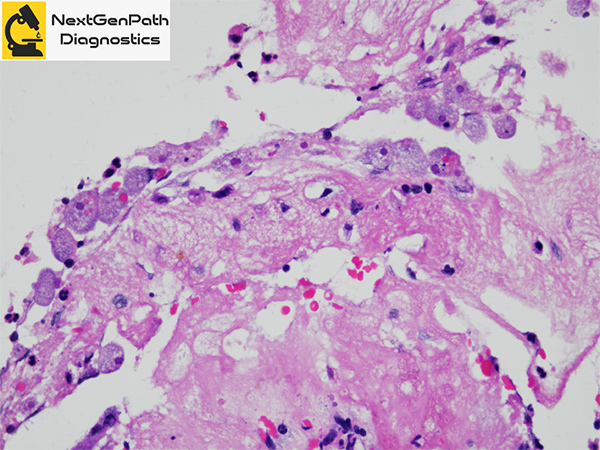
Histopathology: Amoebic invasion through the mucosa and submucosa is the hallmark of amoebic colitis. Lateral extension through submucosal tissues gives rise to the classic flask-shaped ulcer of amoebiasis.
Complications: Fulminant amoebic colitis with perforation peritonitis, ameoboma (mimics malignancy), liver abscess, lung abscess and brain abscess.
Treatment: Metronidazole is the mainstay of therapy for invasive amebiasis. Tinidazole has been approved by the US Food and Drug Administration (FDA) for intestinal or extraintestinal amebiasis.
References
Stanley SL Jr. Amoebiasis. Lancet. 2003;361:1025-34.