In 1963, Boley et al. provided the first detailed histologic description of the most common form of colonic ischemia, resulting from reversible vascular occlusion.
Martson et al. coined the term "ischemic colitis (IC)" to describe this entity.
Enterocolonic ischemia typically presents in elderly patients and is associated with several risk factors, including hypertension, diabetes mellitus, coronary artery disease, peripheral vascular disease, atrial fibrillation, chronic renal disease and hemodialysis.
Patients with irritable bowel syndrome and chronic obstructive pulmonary disease are also at an increased relative risk for gastrointestinal ischemia.
Manifestations of ischemic injury to the gastrointestinal tract are variable.
Only 10% of patients present with gangrenous colitis, whereas most other patients have transient colitis (44%), reversible colopathy (26%), chronic segmental colitis or strictures (18%), or fulminant colitis(2.5%) all of which may simulate other diseases.
The colon, particularly the splenic flexure and descending colon, is more commonly affected by ischemic injury than the small bowel; isolated right colonic ischemia accounts for 10–25% of cases and carries a significantly worse prognosis compared to that in other parts of the colon.
Endoscopy has become the gold standard for diagnosis due to its ability to visualize early mucosal changes. The pathologic findings on biopsies are helpful in confirming the diagnosis and excluding other potential diagnostic considerations.
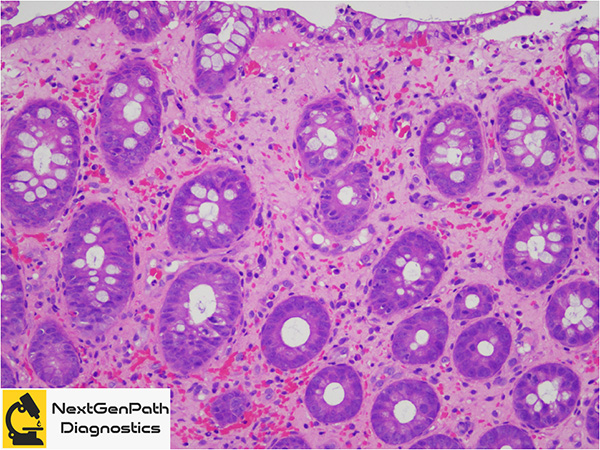
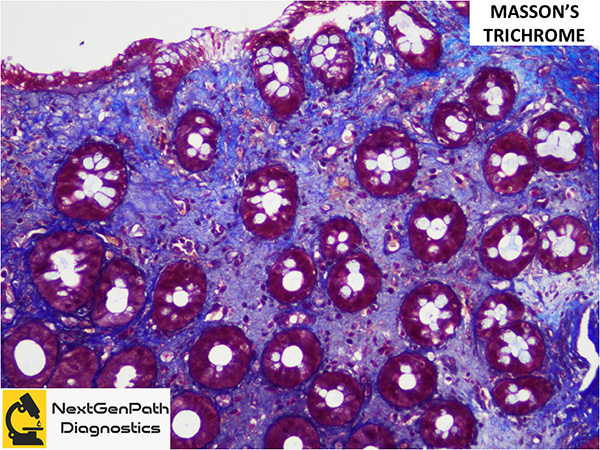
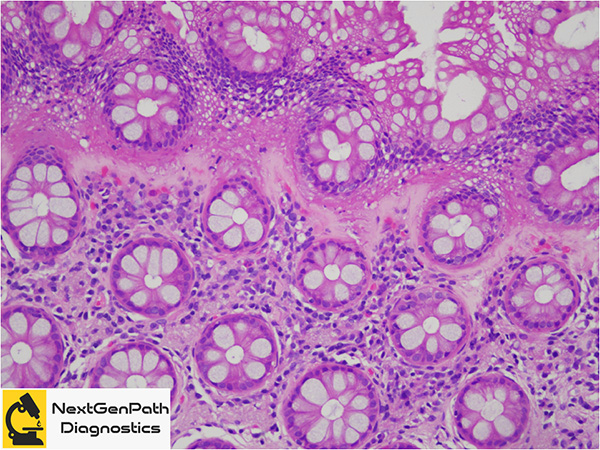
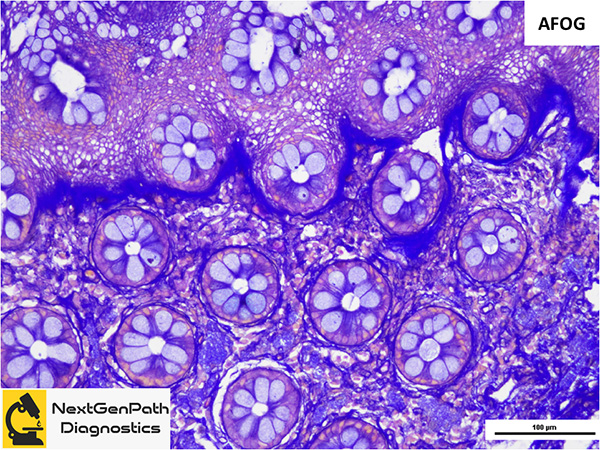
Biopsy: The histologic features of IC have been historically divided into three different stages: the acute phase, the healing and reparative phase, and the chronic phase. Most mucosal biopsies show both acute and reparative changes. Acute phase is characterized by oedematous mucosa with lymphocytes and neutrophils. Additional findings include erosion, superficial ulceration, glandular necrosis more pronounced in the surface with sparing of the deeper portions of the crypts, granulation tissue with crypt abscesses, haemorrhage in the lamina propria, pseudomembranes and inflammatory polyps. Chronic phase shows mucosal atrophy, granulation tissue, and abundant fibrous tissue with iron-laden macrophages. Nuclear regenerative atypia may be prominent. The differential diagnosis of ischemic colitis includes Clostriduim difficile colitis, colitis due to enterohemorrhagic Escherichia coli, drug-induced lesions such as NSAIDs, collagenous colitis, radiation colitis and Crohn’s disease.
Treatment and prognosis: Depends entirely on the underlying etiology of the ischemia as well as the severity of disease process.
References
Uberti G, Goldblum JR, Allende DS. Ischemic enterocolitis and its differential diagnosis. Semin Diagn Pathol. 2014;31:152-64.
Cerilli LA, Greenson JK. The differential diagnosis of colitis in endoscopic biopsy specimens: a review article. Arch Pathol Lab Med. 2012;136:854-64.
Patil DT, Odze RD. Biopsy diagnosis of colitis: an algorithmic approach. Virchows Arch. 2018;472:67-80.