Peripheral Nerve T-Cell Neurolymphomatosis
- Neurolymphomatosis (NL) is defined as infiltration of cranial nerves and peripheral nerve roots, plexus, nerves by lymphoma.
- Most often it is a secondary involvement in a patient with a known diagnosis of lymphoma esp. non-Hodgkin lymphoma.
- B-cell NL is more common than T-cell NL.
- Presentation: most commonly, painful polyneuropathy or polyradiculopathy, followed by cranial neuropathy, painless polyneuropathy, and peripheral mononeuropathy.
- In rare instances of primary NL, the diagnosis is often delayed as it requires integration of clinical information, hematologic work-up, imaging findings (MRI and PET scan), and histopathological examination of involved nerve.
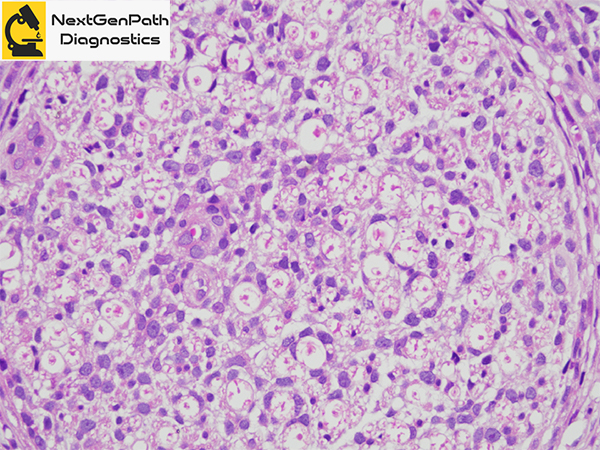
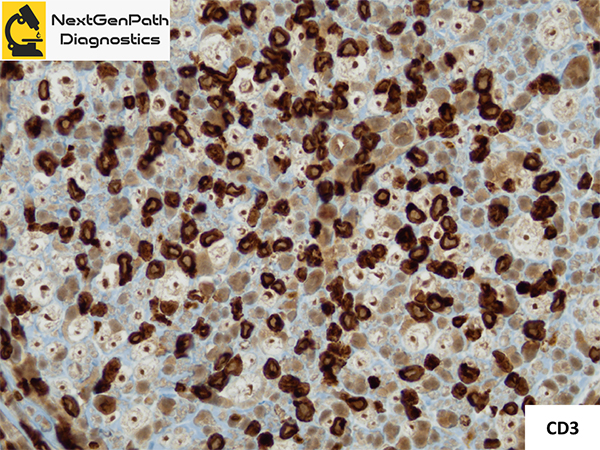
- Histopathological features: a diffuse infiltration of all peripheral nerve compartments by uniform population of atypical lymphoid cells is most typical of NL, although fascicles may be differentially involved. Mitotic figures, pleomorphism, and atypia of the infiltrating cells are highly suggestive of NL. Immunohistochemisty and molecular studies are confirmatory.
- Management depends upon recognition of the disease and its exact neuroanatomic localization without delay.
- Overall, the prognosis appears to be poor.
References
- Li V, Jaunmuktane Z, Cwynarski K, Carr A.Diagnostic delay in a case of T-cell neurolymphomatosis. BMJ Case Rep. 2019;12. pii: e232538. doi: 10.1136/bcr-2019-232538.
- Shree R, Goyal MK, Modi M et al. The Diagnostic Dilemma of Neurolymphomatosis. J Clin Neurol. 2016;12:274-81.
- Baehring JM, Batchelor TT. Diagnosis and management of neurolymphomatosis. Cancer J. 2012;18:463-8.
- Cheung C, Lopes D, Hung KN et al. Neurolymphomatosis: role of positron emission tomography in diagnosis.
- GYL Midroni, JM Bilbao. Biopsy diagnosis of peripheral neuropathy. Springer, Cham. 2015.