Tendency to affect maternal half-siblings but not paternal half-siblings and recur in the subsequent pregnancies.
Multiple unaffected infants prior to having an affected infant (recurrence pattern defy genetic explanation).
Female survivors of NH have healthy unaffected infants.
Tissues (pancreas, salivary glands etc.) affected by siderosis express ZIP14, a known and an excess of circulating non-transferrin bound iron (NTBI) transporter.
Tissues (reticuloendothelial system) that are unaffected by siderosis express ferroportin, which permits iron export.
Associated with renal hypoplasia with dysgenesis of proximal tubules.
Needs multidisciplinary team effort for diagnosis and management.
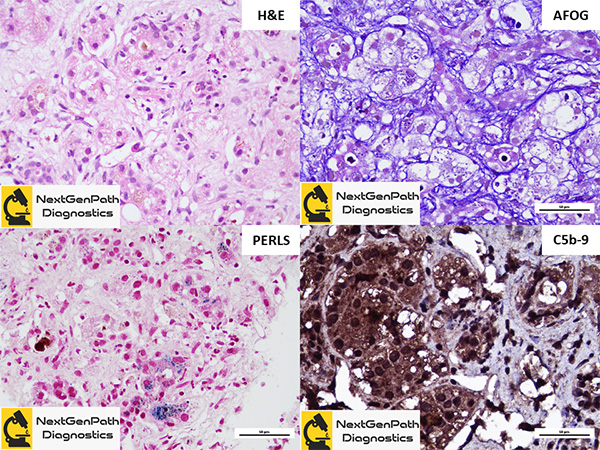
Liver biopsy: Panlobular fibrosis in areas of hepatocyte dropout, degenerative and regenerative changes in the viable hepatocytes - feathery degeneration, multinucleation, pseudoacinar transformation and ductular metaplasia resembling ductal reaction, minimal inflammation, preservation/sparing of portal tracts by the disease process, diffuse intracytoplasmic hemosiderin accumulation in the viable hepatocytes, diffuse hepatocytic staining of complement membrane attack complex (C5b-9). Absence of the following: non-iron storage material in the hepatocytes, excess iron in Kupffer cells, viral cytopathy and in the viable hepatocytes and hemophagocytosis.
Prevention: Recommendation is that subsequent pregnancies be treated with 1 g/kg body weight (maximum 60 g) of IVIG at 14 weeks, 16 weeks, and then weekly from the 18th week of pregnancy until the end of gestation.
Treatment: First line: Double-volume exchange transfusion (to remove existing reactive antibody) followed immediately by administration of IVIG (1 g/kg) (to block antibody induced complement activation). Supportive medical therapy: Combination of antioxidants (vitamin E, selenium, and N-acetylcysteine), membrane stabilizers (prostaglandin E1), and iron chelators (deferoxamine).
Liver transplantation: When all the measures fail.
Prognosis: Generally poor. However, survival into adulthood is reported.
Bonilla S, Prozialeck JD, Malladi P, et al. Neonatal iron overload and tissue siderosis due to gestational alloimmune liver disease. J Hepatol. 2012;56:1351-5.
Zoller H, Knisely AS. Control of iron metabolism--lessons from neonatal hemochromatosis. J Hepatol. 2012;56:1226-9.